Treatment Of Urinary Incontinence In Men
Why do men leak urine?
Urinary incontinence can occur in men for many reasons. Some of these reasons are
- An enlarged prostate
- Prostate surgery
- Neurological condition such as Parkinson’s disease.
I leak urine since my prostate surgery why is that?
The Prostate sits just above the urinary sphincter. When surgery is carried out on the prostate that surgery can damage the sphincter. The sphincter is a ring of muscle which squeezes the urethra and stops urine leaking out. During a TURP (rebore) it is rare for the sphincter to be damaged. During removal of the prostate the sphincter always gets some damage, the amount of damage that occurs depends on your anatomy and the skill of the surgeon.
I leak urine since my prostate surgery will it get better?
Yes, almost always urinary leakage after surgery gets better with time. What you will find is that you will get dry at night first. Then dry in the morning, leaking in the evening is the last thing to come right. This is because the sphincter gets tired working hard all day. Eventually as the muscle gets stronger you will be dry day and night. At the start you will need pads. It is important to stop using pads however when you are dry. So the first step is to stop using them at night, then in the morning and finally get free of your pad totally. It is normal to be worried that you might leak and keep wearing pads “just in case”. The problem is that this makes you lazy and you rely on the pad. It is much better to get rid of the pads if they are not really necessary and your body will work that little bit harder and you should stay dry.
I leak urine since my prostate surgery what can I do?
The first thing to do is practice your pelvic floor exercises. With time and exercises you will get better. Secondly just check that the leakage is when you stand or cough. Sometimes the leakage can be because of urgency, in which case ask your doctor for some medicine, it may help.
How do I do my pelvic floor exercises?
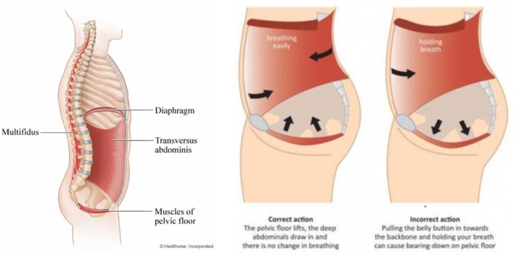
The pelvic floor muscles form 2 slings which pass from the sacrum at the base of your spine to the pubic bone at the front and go around the rectum and the urethra. Theses muscles are fixed out to the sides of the pelvis as well. The idea of a pelvic floor contraction is to squeeze and lift. In men one way to to think this through is to try and lift or flick your penis up. If you do this properly you should feel your anal ring (bum hole) tighten and maybe your scrotum pulls up. You are not trying to hold your breath or tighten your tummy. If you squeeze your tummy you will push urine out rather than keep it in. This is a common mistake in men. You should do both quick (1/2 to 1 second) and long contractions (2-3 seconds). Because the pelvic muscles are attached to the pelvis when you contract then the pelvis will try and tip or move. You can think of this as scaffolding. So for the contractions to work well we need the framework or scaffold to be stable. this can be achieved by strengthening your core muscles. If your core is strong then the pelvis is stabilised and the exercises work better. . When you practice your exercises remember a few important points
- When you train any other muscle for strength you train usually once a day to fatigue, with the occasional recovery day. The same goes for your sphincter. So you should do repeated exercises until fatigue once a day, no more. So one training session a day, no more.
- When you train you need to do 2 types of exercises. The urinary sphincter has fast twitch and slow twitch fibres in it. Fast twitch fibres are rapid on, early off. They activate when you for example cough or laugh. Slow twitch fibres are the slow onset but fatigue resistant. So these work all the time in the background when say you are walking around. So when you do your exercises you need to do some quick penis flicks or pelvic contractions and then some slow strong and hold for 2-3 second type exercises.
- Do not use your tummy muscles. Put a hand on your tummy when you do your exercises to make sure you are not just pulling your guts in. Also don’t clench your butt. This doesn’t help. You can do your exercises either lying down or standing. If you do them standing, then standing pigeon toed stops you co-activating your butt (gluteus maximus).
- You should feel your anal ring (bum) tighten when you do your pelvic exercises. You may also feel your scrotum lift.
I leak with sexual arousal after my prostate surgery. What can I do and will it get better?
Some men, after their prostate is removed, leak urine when sexually aroused. The medical term for this is climacturia, but in fact it can happen either, when you first get an erection, or when you are about to have an orgasm (cum). It usually happens in men who are still leaking urine with physical activity. It will get better with time. As your continence gets better it will happen less and less and should stop. If you are leaking with sexual arousal the options are
- Put a towel on the bed
- Have sex in a place that a little bit of water doesn’t matter e.g. the shower
- Use a penile ring.
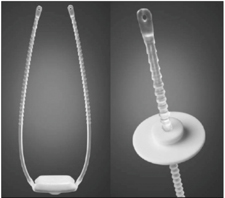
If you place a ring on the base of the penis this will often stop the leakage form happening. You can either use a lasso like device, which can you get through your urologist, or buy one online at http://urosciences.com/blog/urostop-2/ (this is actually a little more expensive), or you can buy a penile ring at a sex shop. These are called “cock rings” at the sex shop.

A urostop, pulling on one limb tightens the soft plastic around the penis and squeezes the urethra shut.
Penile rings can be either just that a soft ring or can be more varied in their shape. They may improve erections, if they are partially occurring already, and may improve sexual enjoyment by your partner as they can push on the clitoris during sex. For more information see http://goaskalice.columbia.edu/answered-questions/considering-cock-rings
I’m still leaking and I’ve tried my Kegel exercises what else can be done?
If the leakage has not settled, then you may need an operation. Before you have an operation you will need to do
- Do a bladder diary and a pad weigh test.
- Have urodynamics
- Have a flexible cystoscopy.
A pad weigh test is a means to assess how much urine is actually leaking. Sometimes what we think is a lot turns out to be not very much. Basically you collect your pad(s) for 24 hours and measure how much extra weight they have. The easiest way to do this is to put a dry pad on your kitchen scales, zero then change for the wet pad. The weight displayed in mg is the amount of urine leaked in mls. Urodynamics are done to make sure that the bladder is not unstable. If so you may get better with pills to calm the bladder down. A flexible cystoscopy is needed to check for two things. One is that there is no scar blocking the bladder (bladder neck stenosis). Secondly it is to check that the sphincter has a good squeeze. If a scar is found that will need to be fixed before any surgery to fix the urine leak. If the sphincter squeezes well then you may be a candidate for an advance male sling. If the sphincter is poor, then an AUS cuff is best.
What type of operations are there?
There are two main operations for urinary incontinence in men. The “gold standard” is an AUS cuff. The newer operation is a sling that pulls up on the urethra. This is called an Advance male sling.
Several other operations are available. Some have already failed or are due to be thrown out as not very good. Some are becoming popular, but are yet to prove themselves as good as either the AUS cuff or the Advance sling.
The basic concept of an AUS cuff is to squeeze the urethra closed at rest and then remove this squeeze when you want to pee. The Advance sling has new concept that incontinence after surgery is in part to the sphincter having “dropped” or being unsupported. The Advance sling aims to “reposition” or support the urethra, rather than compress the urethra using mesh.
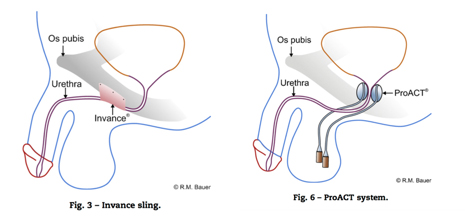
Several other operations all work by various means of squeezing or compressing the urethra. They do this all the time, which seems wrong. They also tend to use large soft surfaces to do this, which should theoretically increase the risk of infection. The more silicon you have around the greater the risk of infection. The INTACT device has already been dropped. ACT balloons are also on the way out, while the ATOM and ARGUS are new compressive devices, and have not been around very long.
What is an AUS cuff?
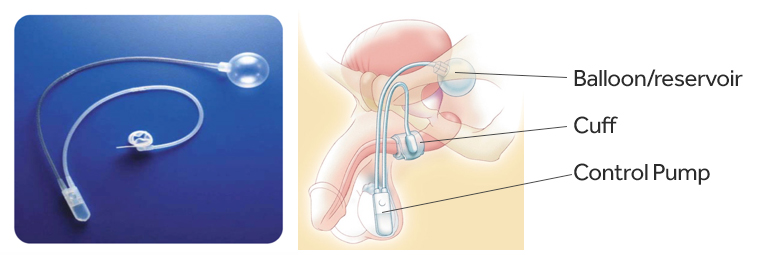
This device has been around for a long time. It is very successful and reliable. At surgery a cuff is placed around the urethra (the pee tube). This is connected to a small balloon which pressurizes the cuff up. So the cuff, at rest, is full of fluid and squeezes the urethra closed. A control pump is placed in the scrotum. Squeezing the pump pumps fluid out of the cuff back to the balloon. The cuff deflates and you can pee. The fluid slowly leaks back and the cuff reinflates.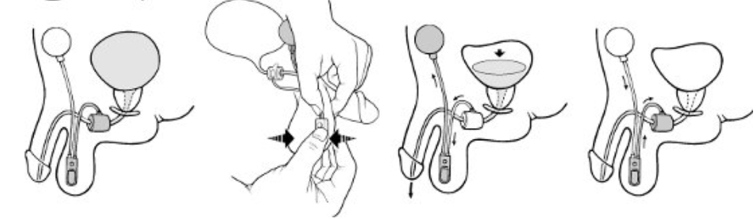
At rest the cuff is inflated squeezing the urethra and keeping the patient dry. When you want to pass urine the control pump in the scrotum is squeezed and this forces water out of the cuff into the reservoir. You can now pee. Once you have finished peeing the cuff reinflates and squeezes the urethra shut again.
When the AUS cuff is first put in, it is left open or “not activated”. This is to allow the urethra to heal. 6 weeks after your surgery you will see me and have the pump activated. This is done by pushing quite hard on a little button on the side of the control pump. This turns on the system and now squeezing the bulb will empty the balloon.
What can go wrong with an AUS cuff?
AUS cuffs have a low failure and complication rate. Three basic things can go wrong. The first is one of the parts or components stops working. This is very rare. The system can get infected. This is also very rare. Finally, the commonest problem is that the pee tube (urethra) under the cuff gets thin and the cuff no longer fits snugly around the urethra. If this happens a new cuff may need to be placed. Extremely rarely the cuff erodes or cuts through into the urethra. IF this happens it needs to be removed. This usually happens if the patient has had radiotherapy as well as surgery for their cancer. It is a good idea to wear a medic alert bracelet warning people that you have a cuff in.
IF someone goes to put a catheter in you then they must call a urologist and deactivate your cuff.
If they do not do this, then the cuff can erode and the system is wrecked (buggered).
It is a good idea to wear a medic alert bracelet warning people that you have a cuff in.
What is an advance male sling?
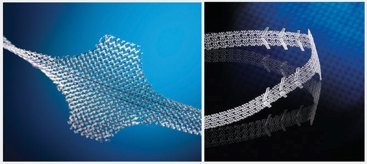
An Advance male sling is a mesh sling that elevates the tissue behind the urethra. It is placed at surgery by passing a mesh tape through the obturator fossa. It is then sutured to the muscle layer around the urethra. When the mesh is pulled tight it pulls this muscle up and this creates bulk around the urinary sphincter. For reasons that are not clear this elevation, rather than compression restores continence. The material is similar to the transoburator tape used in women but the mechanism of action seems different, in that it is not compressing the urethra.
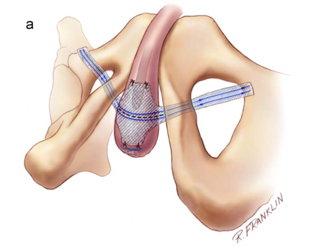
a. the tape is placed across the bulb of the urethra and brought out through the obturator fossa.
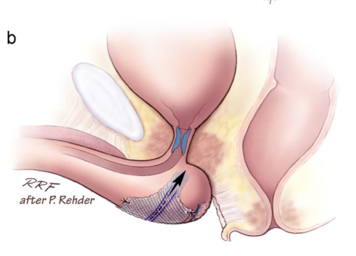
b. The tape is then pulled up parallel to the last part of the urethra (membranous).
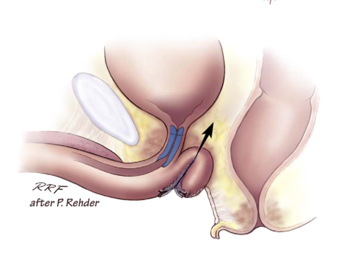
c. This lifts the muscle and tissue up and supports the sphincter.
Who is most suitable for an Advance male sling?
Men who have had a radical prostatectomy and have mild to moderate stress incontinence. You should not need a pad at night, and should leak no more than 150-200mls per day. The ideal candidate is one that is almost dry and leaks with a particular activity, such as bending down or standing up.
What test do I need before an Advance male sling?
In general, you should ? Be dry at night ? Have a flexible cystoscopy and confirm that the sphincter is working well ? If you have had radiotherapy, then the flexible cystoscopy will also check that the urethra is not too white (lacks a blood supply) and instead is nice and pink. ? Have urodynamics. This is a test to check the pressure that you leak at. Ideal candidates for a sling are men who leak at high pressures or not at all during the urodynamic test. On cystoscopy we can see the sphincter closes, in this patient an AdVance sling should work. In this urethra, the tissue looks very pale. This is from radiotherapy damage to the blood vessels, a sling would be a bad idea in this patient.

On cystoscopy we can see the sphincter closes, in this patient an AdVance sling should work.

In this urethra, the tissue looks very pale. This is from radiotherapy damage to the blood vessels, a sling would be a bad idea in this patient.
What can go wrong with an Advance male sling?
The main problems are
- Doesn’t work
- Can’t pee
- Infection
- Erosion
For most men the Advance male sling works really well. The trick is to choose the right person for the operation. Sometimes you may not be able to pee after the operation. If this happens a catheter will be put in to drain the bladder. This will stay in for a week. If you cannot pee at one week, you will be taught self catheterisation. If you still cannot pee after a few weeks, the tape can be loosened. This is very rare.
Sometimes the tape does not work. Again this is very rare. The commonest problem is you still leak a little, that is the operation is not perfect. Very rarely the tape can become infected and very very rarely the tape may erode into the urethra. This is theoretically possible, but has not yet been reported.
Which operation is the best for my incontinence?
That depends on your degree or amount of incontinence. If your leakage is light and especially if it is associated with movement or a specific activity, then the Advance is best. If you leak at night you must have an AUS cuff. If leakage is heavier (say more than 200mls/day) or you leak all the time, then again the AUS cuff is probably best.
If I have surgery can I throw away my pads?
Yes, and No. If the Advance sling works, then you will be completely dry. NO pads. IF you have an AUS cuff then you will be much better, usually one light pad a day. NO pads at night. But not perfect. This is because the cuff cannot squeeze the urethra really really tight, else it will cut off the blood supply. The maximum squeeze pressure in the cuff must be below your mean blood pressure so that the urethra is not ischaemic. So when you cough or sneeze or lift you rise the pressure in the bladder above your mean blood pressure and a little will leak. Attempts have been made to create a second mechanism to compensate for this rise in pressure, but so far they have not worked.
If the AUS cuff will not make me dry why put it in?
The problem is this. The advance sling makes your sphincter work better, but does not replace it. So if you have heavy leakage, and particularly if you leak at night then the sphincter is too weak, and the Advance sling will not work at all. But if you have light leakage then the sphincter when “repositioned” can work and you can be completely dry. No one solution is perfect and no one size fits all.
Will I be dry afterwards?
That depends on the amount of leakage you had before surgery and the operation you had. Men who leak a lot are much better, but usually not cured. Men who leak a little are usually cures.
What other operations are there?
There are at least three operations that should not be done anymore. These are the InVance, the ACT balloon and TOMS. All are compressive systems which have not worked well. Two new systems which are still being assessed are the ATOMS and the ARGUS. Again both are passively obstructive, have short follow-up histories and likely will not be as good as an AUS cuff and will cause more blockage and risk of an infected system that an Advance sling. Both are yet to have long term success rates published. The AUS cuff was developed precisely because pure compressive devices acting on the urethra worked well in the short term but not in the long term. See for more information http://www.medscape.com/viewarticle/540085
In the AMOS system a big flat pad of silicone is pulled up against the urethra and tension is adjusted using buttons which click lock on the suspension limbs.


In Atoms a compressive inflatable pad is placed against the urethra and wrapped with mesh into place. The pad can be inflated until continence is achieved. This is both a positive and a negative, since such manipulation increases the chance of infecting the system.
Compressive bulbar urethral slings in men are, in my opinion never a good idea in the long run! ?
In Summary:
From Contemporary Management of Postprostatectomy Incontinence. Bauer RM, Gozzi C, Hubner W et al. European Urology 59(2011) 985-996.