Bladder Cancer
What is bladder cancer?
Bladder cancer is a tumour that grows from the inside lining of the bladder. The lining of the bladder is called the transitional epithelium and almost all bladder cancers grow from this layer. Bladder cancers are therefore usually called transitional cell cancers or TCC’s.
Are all bladder cancers the same?
No. Bladder cancers can differ in the type of cell found and in the depth of invasion present.
More than 90% of bladder cancers are called TCC’s that is they arise from the lining cells of the bladder. Much less commonly the cells that make up the cancer are from other cell lines. These will not be discussed here.
Thankfully most bladder cancers are very superficial. That is they grow just on the surface of the bladder lining. It is uncommon for a TCC to grow deeply into the bladder wall.
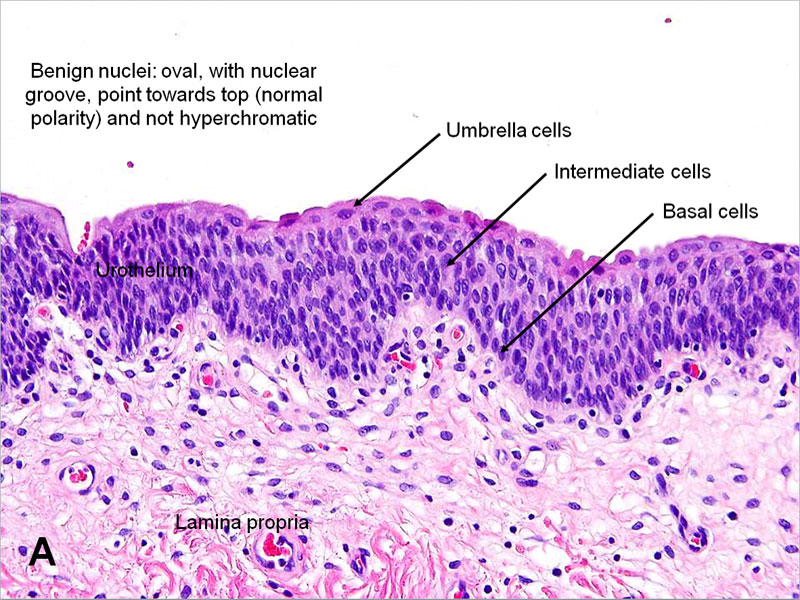
Normal Bladder wall lining
What does the Stage or depth of the cancer mean?
Most cancers are TCC’s, and they grow on the surface of the inside of the bladder. When we look at bladder cancers we are most interested in whether the cancer is just growing on the surface or has started growing from the surface down into the wall of the bladder. Luckily 4 out of 5 bladder cancers grow just on the surface.
Bladder cancers which grow just on the surface are called superficial cancers. They can be quite large but despite this they do not send roots into the bladder wall. They are therefore very unlikely to spread around the body. They do however like to reoccur or come back, so follow-up is needed. Almost all superficial cancers are low grade.
About 10% of cancers grow into the wall of the bladder. This is a sign of invasion. The bladder wall has three layers to it. A superficial waterproof lining, a thick outer muscle wall and a thin layer between the inner waterproof lining and the muscle. This in-between layer is called the lamina propria and probably is where the bladder senses and controls its function from. Cancers that are confined to the lining are called Ta, those into the next layer T1, and if into the muscle this is called T2. Cancers that extend through the muscle wall into the fat outside the bladder are called T3 disease.
A third type of TCC is called Carcinoma-in-situ or CIS. This is a special variant of superficial cancer, which forms very thin patchy cancers throughout the bladder lining rather than a discrete lumpy cancer. Although these cancers only affect the very superficial layer of the bladder they are much more likely than other superficial cancers to become invasive. They are therefore treated much more aggressively than the standard type of superficial cancer (Ta).
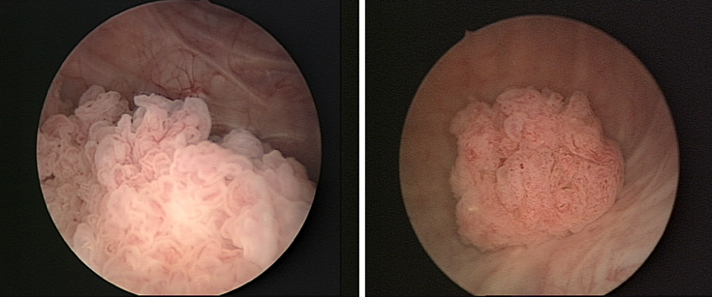
A low-grade bladder cancer growing on the inner surface of a bladder
About 10% of cancers grow into the wall of the bladder. This is a sign of invasion. The bladder wall has three layers to it. A superficial waterproof lining, a thick outer muscle wall and a thin layer between the inner waterproof lining and the muscle. This in-between layer is called the lamina propria and probably is where the bladder senses and controls its function from. Cancers that are confined to the lining are called Ta, those into the next layer T1, and if into the muscle this is called T2. Cancers that extend through the muscle wall into the fat outside the bladder are called T3 disease.
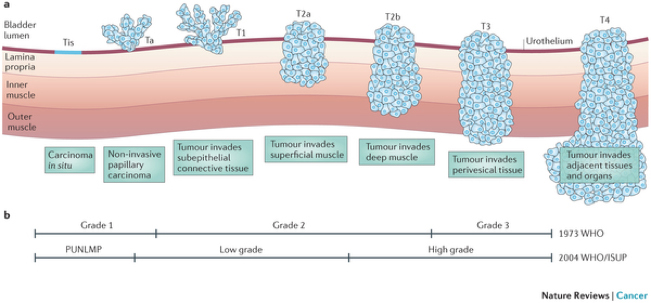
Stages of bladder cancer: Superficial cancers grow on the surface. Invasive cancers grow into or through the bladder muscle.
A third type of TCC is called Carcinoma-in-situ or CIS. This is a special variant of superficial cancer, which forms very thin patchy cancers throughout the bladder lining rather than a discrete lumpy cancer. Although these cancers only affect the very superficial layer of the bladder they are much more likely than other superficial cancers to become invasive. They are therefore treated much more aggressively than the standard type of superficial cancer (Ta).
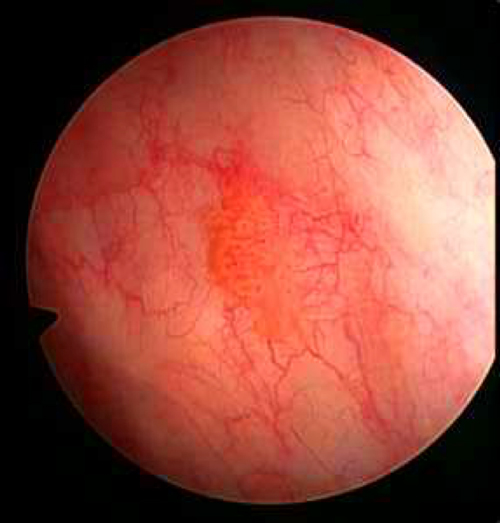
CIS appears as a flat red patch on cystoscopy
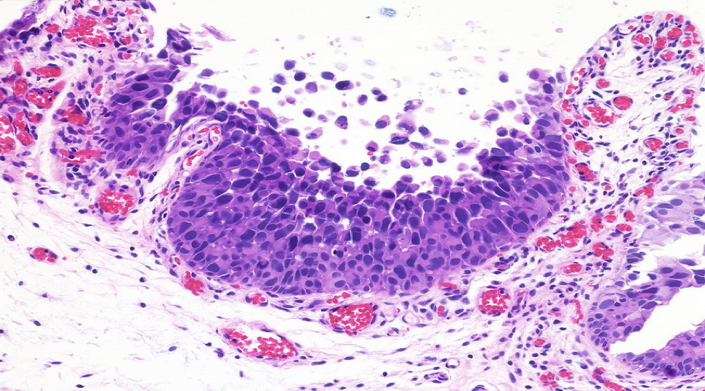
In CIS the cancer cells do not stick together but float off into the urine
What causes bladder cancer?
Bladder cancers occur because of chemicals in the urine that have damaged the lining of the bladder over decades. This means that the whole lining of the bladder has been affected and only a small area at any one time grows a cancer. Smoking is the most common preventable cause of bladder cancer. Very rarely other industrial chemicals can cause bladder cancer. Most of these chemicals are now banned.
Because the most concentrated urine sits at the bottom of the bladder most initial cancers are on the floor or sides of the bladder. Also when we remove a cancer some of the cancer cells can spread around the bladder. These can stick to the bladder lining and grow a new cancer. Thankfully these grow like the first cancer, that is only on the surface and eventually all can be eradicated.
What is the difference between recurrence and progression?
Recurrence is when a cancer returns or comes back. Progression is when the cancer grows more deeply into the wall of the bladder or spreads to other organs.
Often when we talk about a cancer the thought that it has recurred or come back would be an awful thing. In bladder cancer this is not the case. Bladder cancers are more like skin cancers. When we get skin cancers removed it is common to have another one occur later. This is because the sun has damaged all the skin that was exposed and the cancers occur at different time intervals.
What are the symptoms of bladder cancer?
Most bladder cancers do not cause any symptoms, and are found when a person is investigated because of microscopic (non visible) blood in their urine. Sometimes bladder cancers present with blood in the urine that can be seen (visible haematuria), occasionally bladder cancers present with urgency and frequency. Most people with frequent urgent passage of urine do not have bladder cancer.
How is bladder cancer diagnosed?
Bladder cancers are diagnosed through x-rays, urine tests and an operation where we look into the bladder (cystoscopy) and cut out the bladder tumour.
The x-rays that are used can be an ultrasound or a CAT scan. Unfortunately x-rays miss a lot of bladder tumours. Urine tests can sometimes be helpful, but usually only work in high grade or nasty cancers. Because of the problems with picking up all bladder cancers with x-rays or urine tests all patients will eventually need a look into their bladder, this is called a cystoscopy.
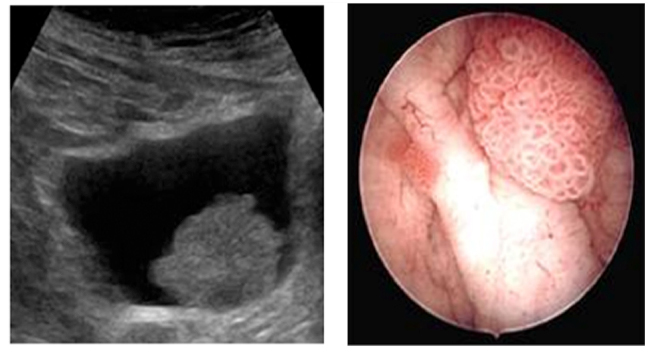
A bladder cancer seen on ultrasound, and the corresponding lesion on cystoscopy
I need a TURBT what is that?
TURBT is the name for the operation which removes a TCC from inside the bladder. It stands for TransUrethral Resection of Bladder Tumour. In TURBT a surgeon looks inside the bladder with a telescope and cuts or scoops out the cancer with a thin metal loop.
After the cancer is cut out a scar is left in the bladder wall, which will eventually heal over with new bladder lining.
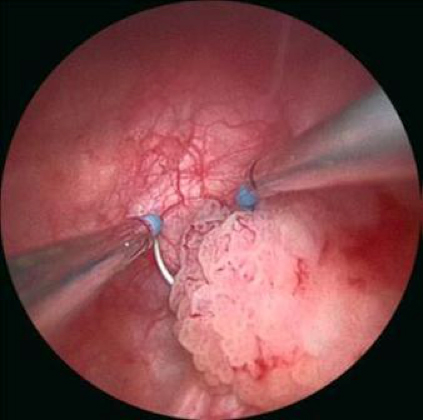
A small bladder cancer just about to be cut out. The loop can be seen behind the cancer
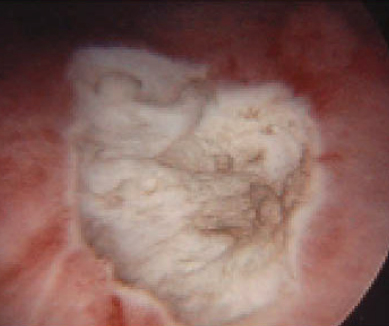
A grey flat wound is left behind. This will heal over in about 6 weeks, leaving a scar.
What happens after my operation?
A catheter is placed into the bladder and salt water is then used to wash out any bleeding that may occur after surgery. The catheter is usually taken out the day after surgery. Sometimes an anti-cancer drug is placed into the bladder the morning after surgery. This may kill any cancer cells that are floating in the urine after surgery. The idea of this is to increase the time it takes to develop a recurrence.
How long do I need follow-up for?
The minimum is 5 years clear of any recurrence. Typically you will have a flexible cystoscopy 3 months after your TURBT. If this is clear then the next cystoscopy is 9 months later. If that is clear then an annual flexible cystoscopy is done until you have achieved 5 years without any recurrence.
If you had a high grade lesion, or CIS or invasive cancer then you should be followed for 10 years.
Do I need more x-rays during follow-up?
IF your original cancer was a superficial TCC (Ta) then no. IF you had CIS or invasive disease then a type of CT scan might be done at 5 years.
Can I have a urine test instead?
The place of urine tests as part of the follow-up of bladder cancer is still not known. The easiest urine tests to do are urine cytology and Cx Bladder. Both tests are good at picking up high grade cancers but poor at detecting low grade cancers. At present they are probably best done as well as rather than instead of a flexible cystoscopy.