Surgery For Female Stress Urinary Incontinence
What types of surgery are offered for stress urine incontinence and why?
Operations for stress incontinence are designed to support either the bladder neck or the urethra during coughing and during other periods of raised abdominal pressure. It is believed that abnormal movement of the urethra, so called hypermobility of the urethra during these periods of raised abdominal pressure is at least partly responsible for incontinence in women.
Over time the operations used have changed as different surgical techniques are tried. All operations have a failure rate over time. Previously operations were done either open, or as a suspension suture operation. The standard open operations up till the early 2000’s was either an open Birch colpo-suspension or a pubovaginal sling. Both were quite invasive operations.
As these were major operations a variety of suspension suture operations such as the Stamey were invented. Over time most of these operations failed. This led to the search for an operation that was less invasive than the open operations but more effective that the suspension suture operations. In approximately 1996 a monofilament synthetic sling was introduced by Johnson and Johnson as the Gynecare-TVT. This was the first effective synthetic sling operation. Since then a raft of different products have been introduced, often without adequate trials and most of these failed or had serious complications. At present the standard mesh slings are a TVT/SPARC tape or a TOT/MONARCH tape. All other tapes should not be used.
The mesh used is the same as that used for hernia repairs, and it was chosen because it was already approved for use in humans (in hernias). It is possible that this is not the best material to be next to the vagina or urethra, but so far, it has worked out the best of all the synthetic materials trialled.
Over recent years concerns over the use of mesh have been raised because of complications such as pain and the risk of the mesh material eroding into the vagina, urethra or bladder. This has lead to a slight swing back towards the pubovaginal sling, but not the Burch colposuspension.
What is a mesh sling tape?
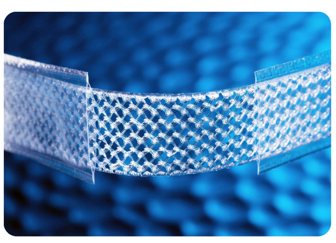
A mesh sling operation uses a piece of synthetic tape to support the middle of the urethra. The tape is made of a non-absorbable material, basically the same material as a non absorbable suture (prolene). As it is non-absorbable it will stay there for ever. A mesh tape is a relatively safe, simple straight forward operation with a high success rate, but over time some successful operations do fail.
Here we can see a mesh close up. As we can see it has an open weave to allow the body to grow into it. This sticks the tape in position. The material is a bit rough and does not dissolve. This may also be why sometimes it erodes as the body reacts to it and tries to get rid of it.
How is the operation done?

In all operations a small cut is made in the skin and a cut is made in the front wall of the vagina. A metal rod called a trocar is then passed through from the skin cut to the vaginal incision. The trocar then has the mesh clipped onto it and the mesh is pulled up on either side of the urethra. A plastic outer sleeve is then pulled off leaving the mesh in place.
Are there different types of mesh sling operations?
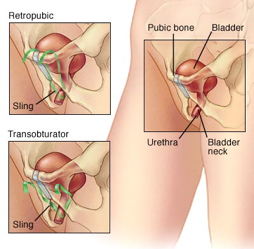
Yes, there are two standard ways to placing a mesh sling. Both pass a sling under the urethra, but they differ on where the sling passes to after that.
In a TVT or SPARC operation the tape passes up and down. That is the tape passes around the urethra and up behind the pubic bone like a U. This is called a retro-pubic operation. A second type of operation, called a TOT or MONARCH, using the same material but passes the sling under the urethra but in a more open V shape. In this operation the “limbs” of the tape pass out sideways to the groin. This is called a trans-obturator operation
What is a TVT or SPARC?
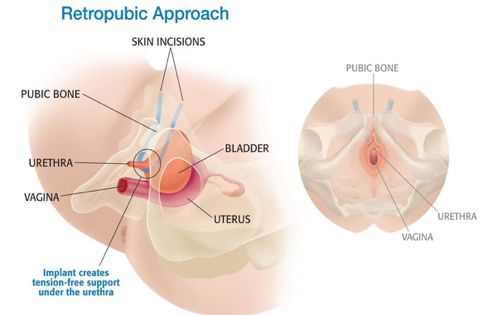
A TVT or SPARC is a mesh suspension sling which passes up behind the pubic bone. IT is therefore called a retro-pubic approach.
In a TVT or SPARC operation the tape passes under the urethra then back up behind the pubic bone. It supports but should not theoretically compress the urethra.
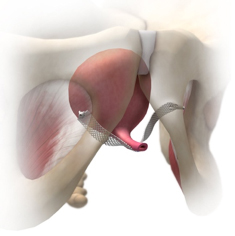
What is a TOT or MONARCH?
In a TOT operation the same mesh is used as in a TVT but now it passes side to side and comes out in the inner thigh. This is less likely to cause a blockage to peeing, but if leakage is moderately severe it may not work.
Which mesh sling operation is better for me?
Both operations support the urethra with a monofilament non-absorbable sling via a relatively minor operation. The TVT holds the urethra in a U while the TOT holds the urethra in an open V. This means that the TVT tends to be a little more effective but more likely to block the urethra, that is the tube you pee through.
Before your operation you would normally have had urodynamics. At that test the pressure at which you leak will have been measured. For women with a high leak point the TOT is best, for women with a medium leak point the TVT is better. IF the leak point pressure is low then neither operation is a good idea.
How long will I be in hospital for after my sling mesh repair?
I night is the usual stay. You will come back from theatre with a catheter in, which will be removed the following morning. Typically, you should be able to pee and then you can go home.
What can I do and what can’t I do after my operation?
It is really really important to not do any heavy lifting for 6 weeks after your surgery. This is to allow the tape to lock itself into position. So you should avoid lifting, vacuum cleaning and probably not drive a car for a couple of weeks. After that be careful what you carry or lift into the boot of the car till the six weeks is up.
When can I have sex after a sling operation?
Because of the cut in the vagina with mesh behind it, you should not have vaginal penetration as part of sex for 6 weeks after your surgery. If you have vaginal penetration before the 6 weeks is up, you may increase the risk of the mesh eroding into the vagina.
What can go wrong with my mesh sling operation?
Most operations go well. The general complications for both types of mesh suspension slings are
-
Can’t pee afterwards
-
Doesn’t work
-
New onset urgency
-
Erosion into the vagina
-
Infection
-
Bruising/haematoma
-
Late erosion into urethra
-
Pain on sex (dyspareunia)
-
In a TVT operation because the tape goes up behind the pubic bone there is a small risk of putting a hole in the bladder while doing this
-
After a TOT you can get thigh pain, where the mesh was put in. This usually settles with injections of local anaesthetic and steroids.
-
A very rare problem is erosion into the urethra (the tube you pee through). It is extremely rare, but if it does occur can lead to devastating complications.
In general, it is rare to have a major problem after the operation. One problem that is sometimes not mentioned is new onset urgency. Some 6-10% of women get the urgent need to pee after this operation. With time it may or may not settle, and it may or may not respond to pills. Significant pain with sex is uncommon. If it odes happen then it may respond to removal of the tape, but not always.
I can’t pee after the operation, what happens now?
If you cannot pee after the catheter comes out on day one postop then you will have the catheter put back in. It will be removed a week later, and most times you will pee ok. If you still cannot pee, then you will be taught how to self catheterise (this is called ISC). With time most people start peeing again. If after a month you are still not be able to pee, then the tape can be cut. When this is done there is a small risk of incontinence coming back.
My tape has eroded into my vagina, what do I do?
Erosion of the tape into the vagina is uncommon, but is the most common of the problems with tape. If this happens it can usually be treated by nightly intravaginal oestrogen cream. If this does not work, then a small operation to close the erosion will be needed. A small amount of the tape may need to be removed at the same time.
Is mesh safe?
Unfortunately, nothing is ever 100% safe. Mesh is very effective at fixing stress leakage, and allows a strong quick operation that you can recover from quickly. But it does have specific problems. As stated above the commonest special complication is erosion, and this usually can be fixed with intra-vaginal cream. To recap however, the specific risks of mesh are
-
erosion into the vagina
-
infection
-
pain on sex
-
pain in the thigh if a TOT was done
-
erosion into the urethra.
What is a pubovaginal sling operation?
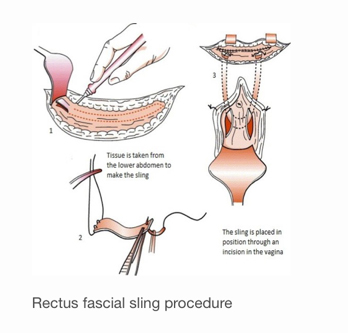
A pubovaginal sling operation is in some ways a little like a TVT but instead of using mesh a piece of your body tissue is used to support the urethra or bladder neck. This piece of tissue is called fascia, and is harvested from your thigh or from your abdomen. This means that usually you will have a big cut in your lower abdomen where the tissue was harvested from. Because the tissue is from your own body it is called an autologous sling. There was a time when surgeons used tissue form dead people (cadaveric graft) or from part of the gut of pigs (small intestinal submucosa), but neither should be used anymore.
When you use a piece of the abdominal fascia to make the sling it is called an autologous sling
It is a bit harder to get the tension of a pubovaginal sling correct, so you are a more likely to have difficulty peeing afterwards. This can get worse with time as the tissues shrinks as it scars. Some people have to put a catheter into the bladder to empty it when this happens. This is called intermittent self catheterisation.
Because of these issues the TVT was invented. However, because of concerns over having mesh inside you there is a small trend back to pubovaginal slings. Unfortunately, nothing is ever perfect.
In a pubovaginal sling operation, tissue is first taken form the front of the abdomen (tummy). A stitch is placed at each end and then the tissue is passed under the urethra.
What can go wrong with my pubovaginal sling?
After all operations you can get a wound infection, haematoma (bruise), urinary tract infection or pain. Wound problems are more common after a pubovaginal sling and you will have more pain afterwards in the wound. This will settle with time. Not being able to pee after the operation is more common after a pubovaginal sling, and in fact you should be taught how to catheterise yourself before having this operation. This is especially true if you have had a previous failed mesh operation. With time most people can pee again, but a minority of women never start peeing again.
To recap the potential risks of a pubovaginal sling are
-
wound pain, haematoma or swelling
-
wound infection
-
Cannot pee and need to catheterise for a period
-
Cannot pee and need to catheterise for the rest of your life
-
A hole in the urethra or bladder neck during surgery (in which case the catheter will be left in for a few extra weeks).
When can I go home after a pubovaginal sling?
In general, you will need to spend 2-3 days in hospital after a pubovaginal sling. This is because the wound can be quite sore and the catheter needs to stay in for 2 days after the operation.
When can I have sex after a pubovaginal sling?
Again, best to avoid vaginal penetration for the first 6 weeks after surgery.
Why would I choose a pubovaginal sling over a mesh suspension sling?
There are 3 reasons to choose a pubovaginal sling over mesh.
-
The commonest reason is severe stress urinary incontinence. This is sometimes called type 3 stress leakage. When you had your urodynamics this would have shown a very low leak point pressure. In this setting a TVT has a higher failure rate than a pubovaginal sling
-
A previous failed mesh operation. Sometimes if the leak point I slow a TVT will be tried. If this fails to work, then a pubovaginal sling will need to be put in. This may mean removing the old mesh and bringing down omentum to wrap around the urethra. The risk of not peeing is higher with this operation than the normal pubovaginal sling.
-
You don’t want mesh inside your body.
How successful is surgery for stress incontinence?
The success rate depends on the degree of incontinence and the definition of success. Is success no pads or is it one light pad? In general, both autologous (using your tummy tissue) and mesh slings have a similar success rate. The American Urology association has estimated the following results for each system.
Mesh mid urethral slings
-
success (dry) 81-84%
-
new onset urge incontinence 6%
-
urinary retention 3%
-
vaginal erosion 7%
Autologous slings
-
success (dry) 90%
-
new onset urge incontinence 9%
-
urinary retention 8%
Useful websites for
http://www.nhs.uk/planners/pregnancycareplanner/documents/bandbf_pelvic_floor_women.pdf
http://physiotherapy.org.nz/your-health/how-physio-can-help/pelvic-floor-disorders/